Workflow Manager
Visualize and optimize your business processes
Build software that fits your business. From simple approvals to complex data manipulation, the Decisions Workflow Manager makes any task faster and more effective.
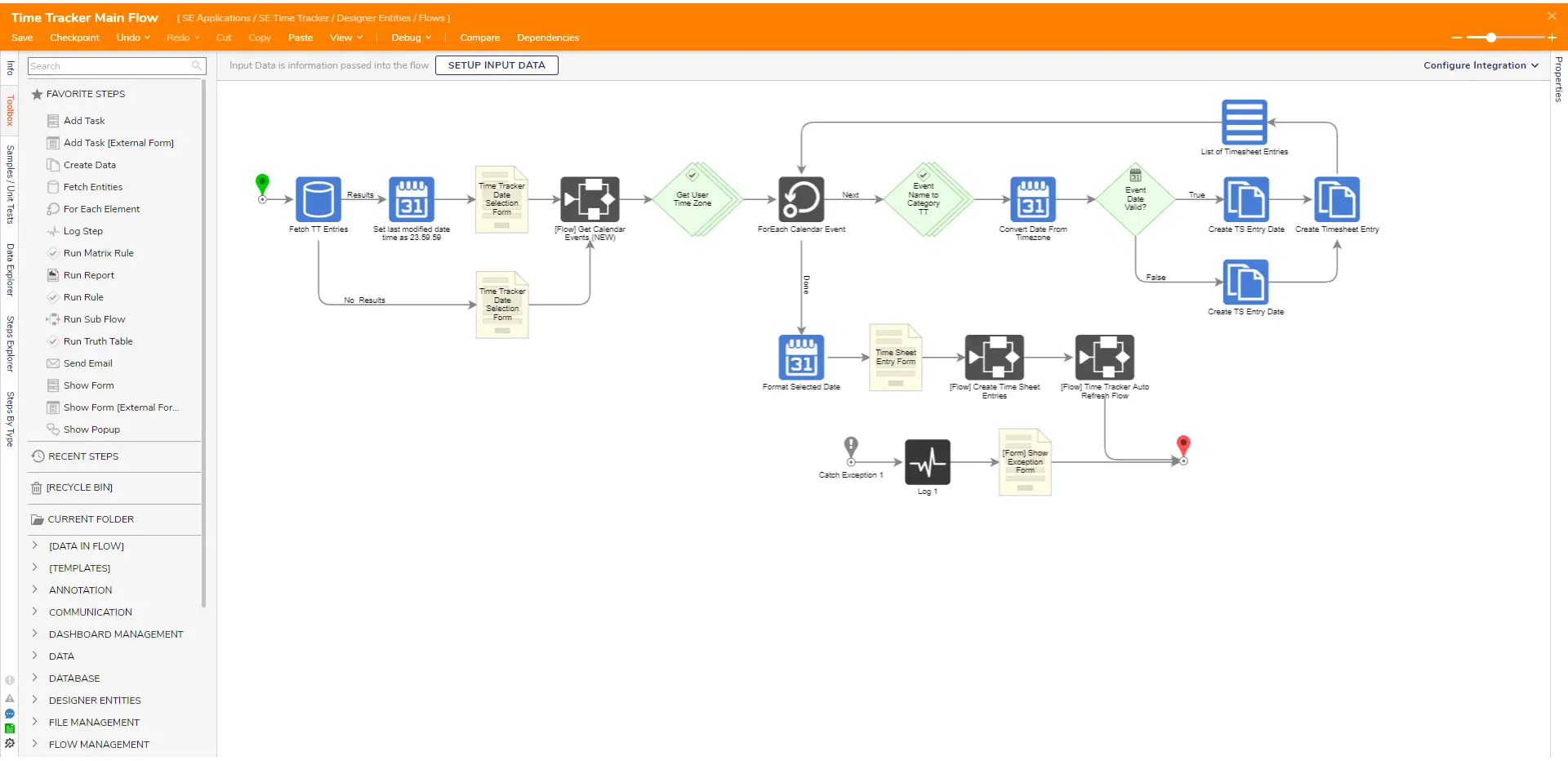
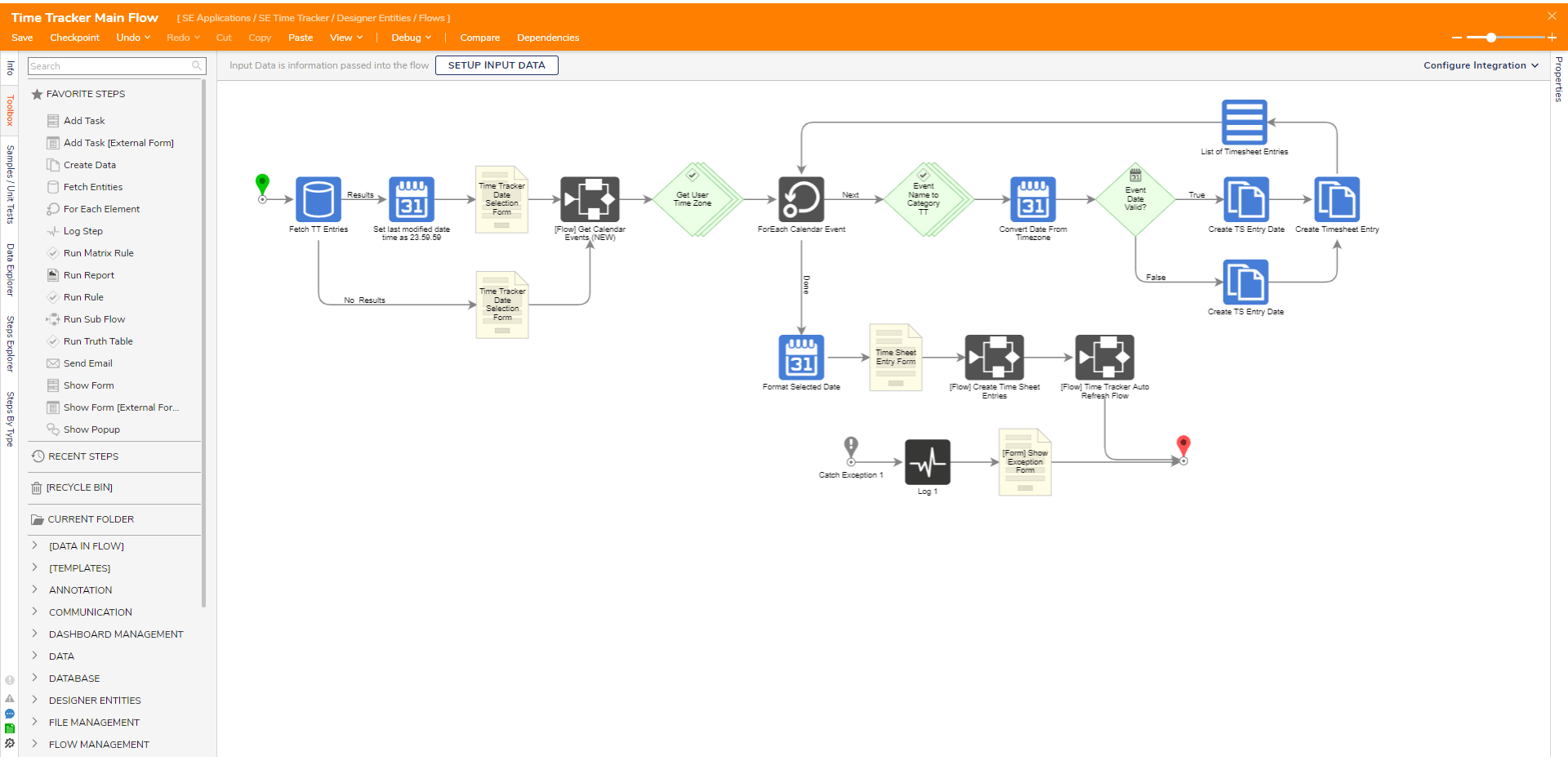
The Decisions Workflow Manager makes any workflow design feel like a whiteboard session with its graphical, no-code interface. Invite your business leaders to collaborate with developers, leveraging their expertise in high-value processes.
Stop relying on spreadsheets to manage your most important processes. The Decisions Workflow Manager simplifies your business automation by digitizing each step and action, without the need for custom code.
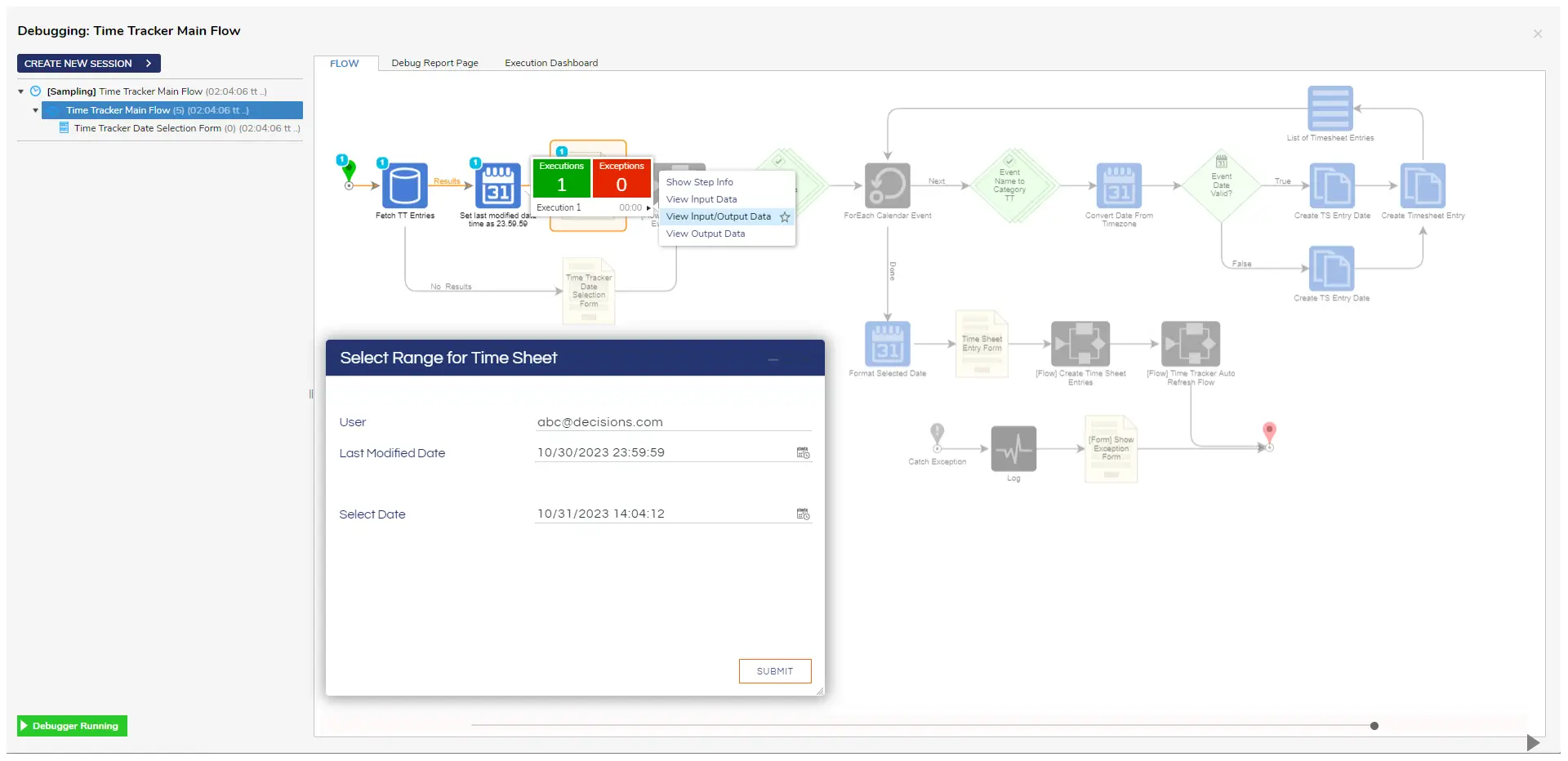
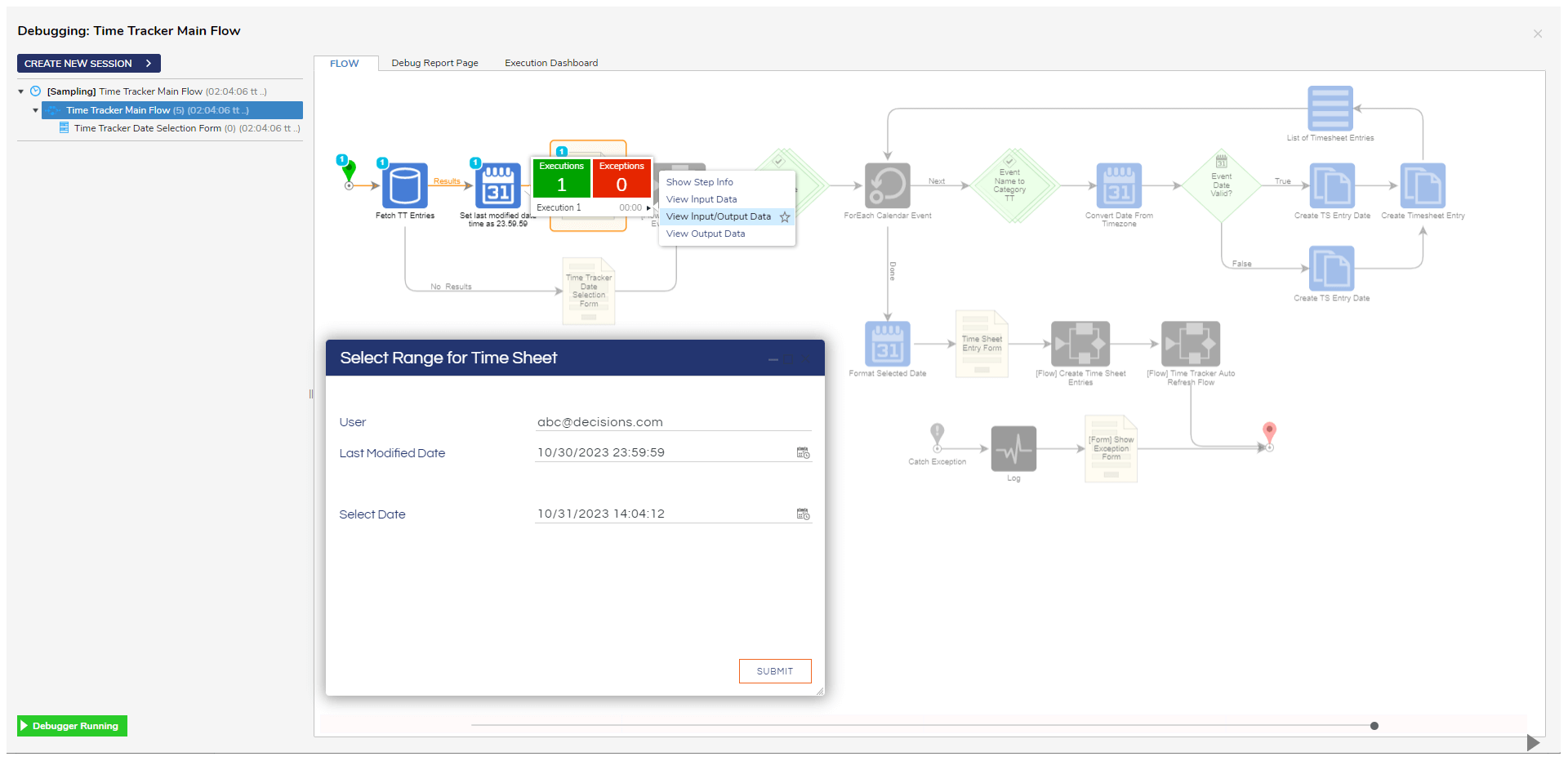
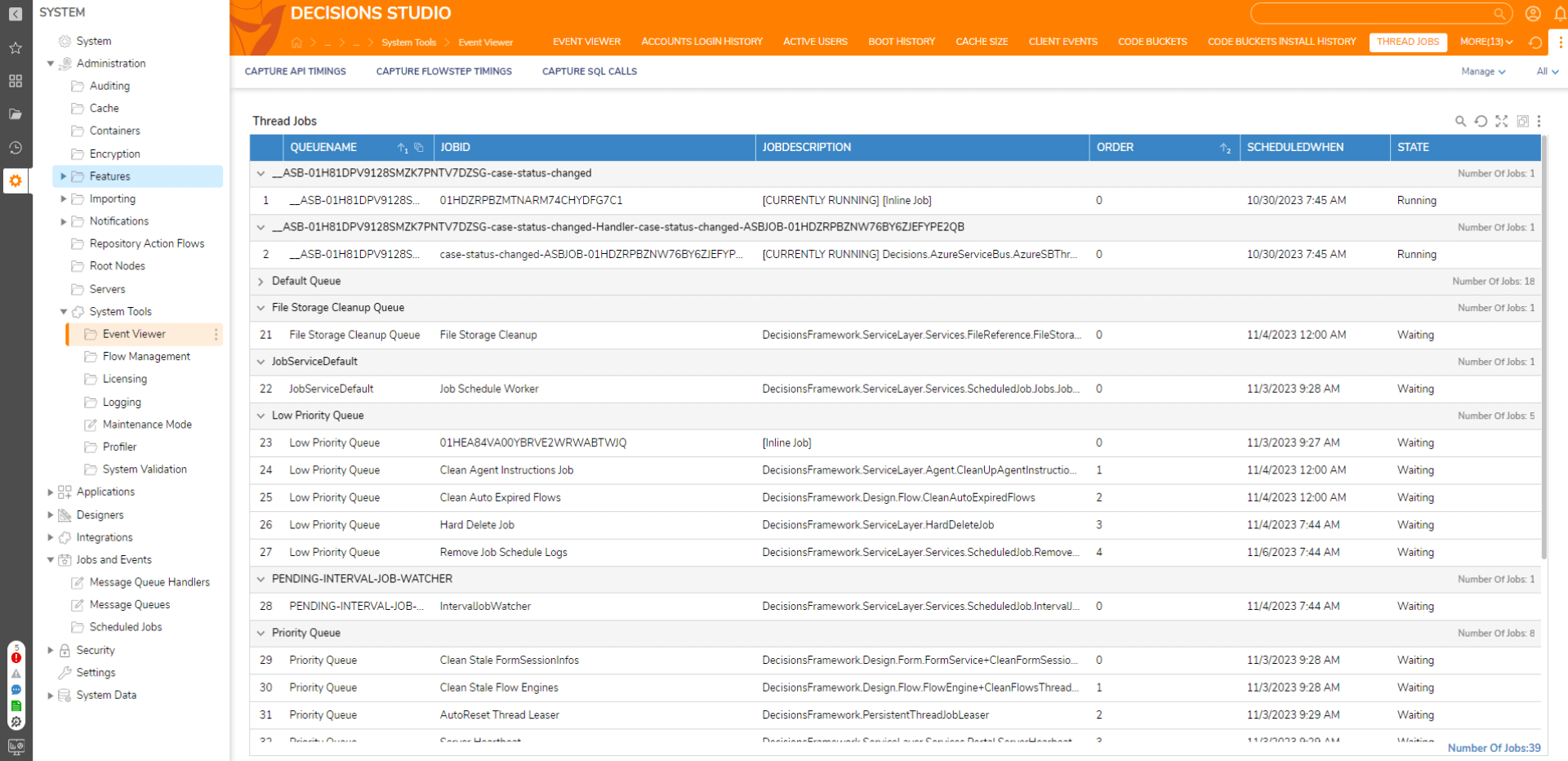
Test and improve as you build. The Workflow Manager provides real-time error notifications and powerful debugging tools to improve efficiency and prevent costly mistakes. Track key metrics to see the business impact of every workflow.
Streamline your modern workflows by incorporating tasks for both employees and computer systems. Utilize the Decisions Workflow Manager to trigger digital and manual actions, optimizing resource allocation and adapting to your business’s dynamic needs.

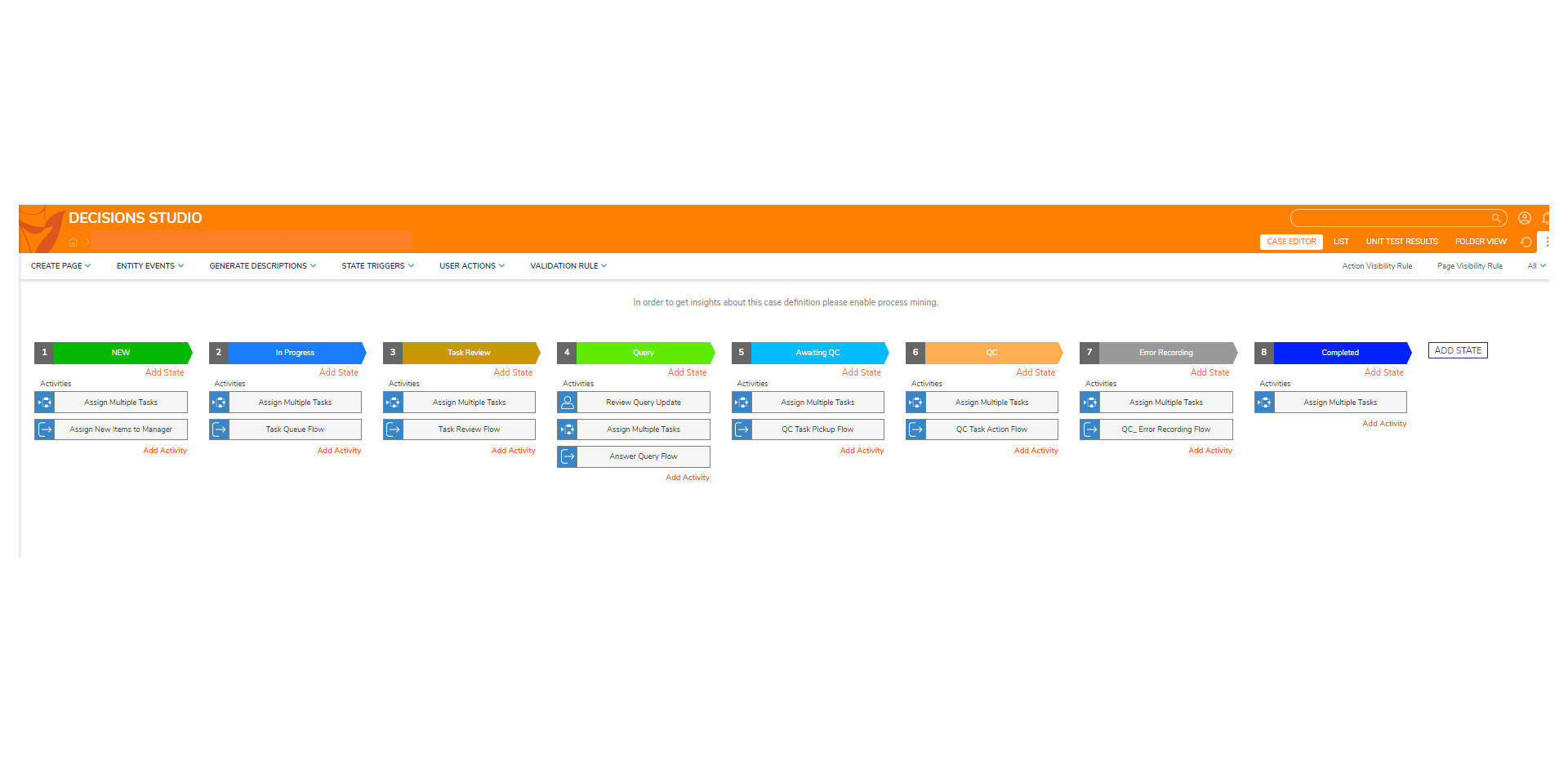
Decisions provides a centralized platform for managing all your work queues. With our user-friendly graphical interface, you can easily assign, prioritize, and monitor work items, ensuring that nothing falls through the cracks.

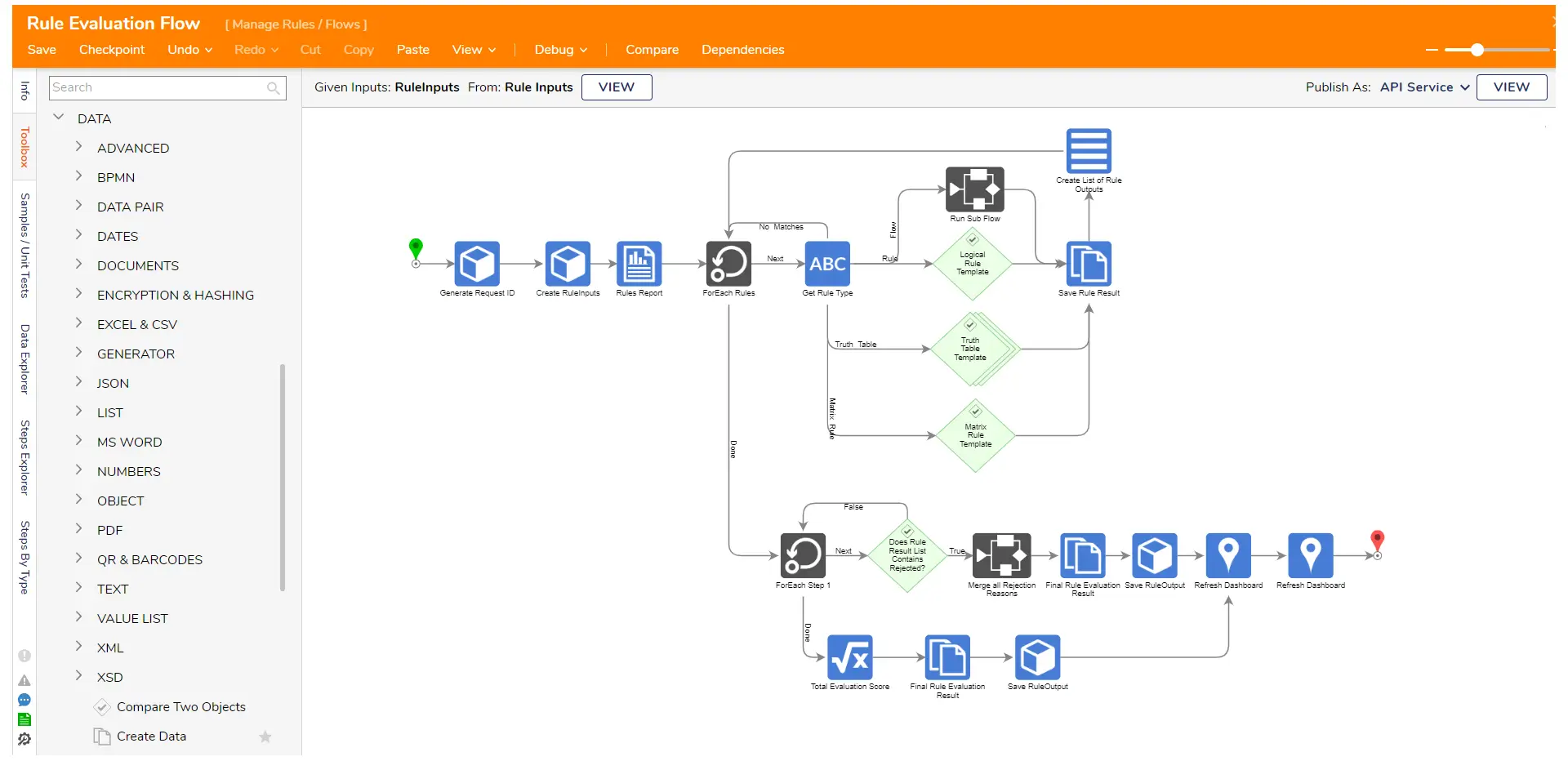
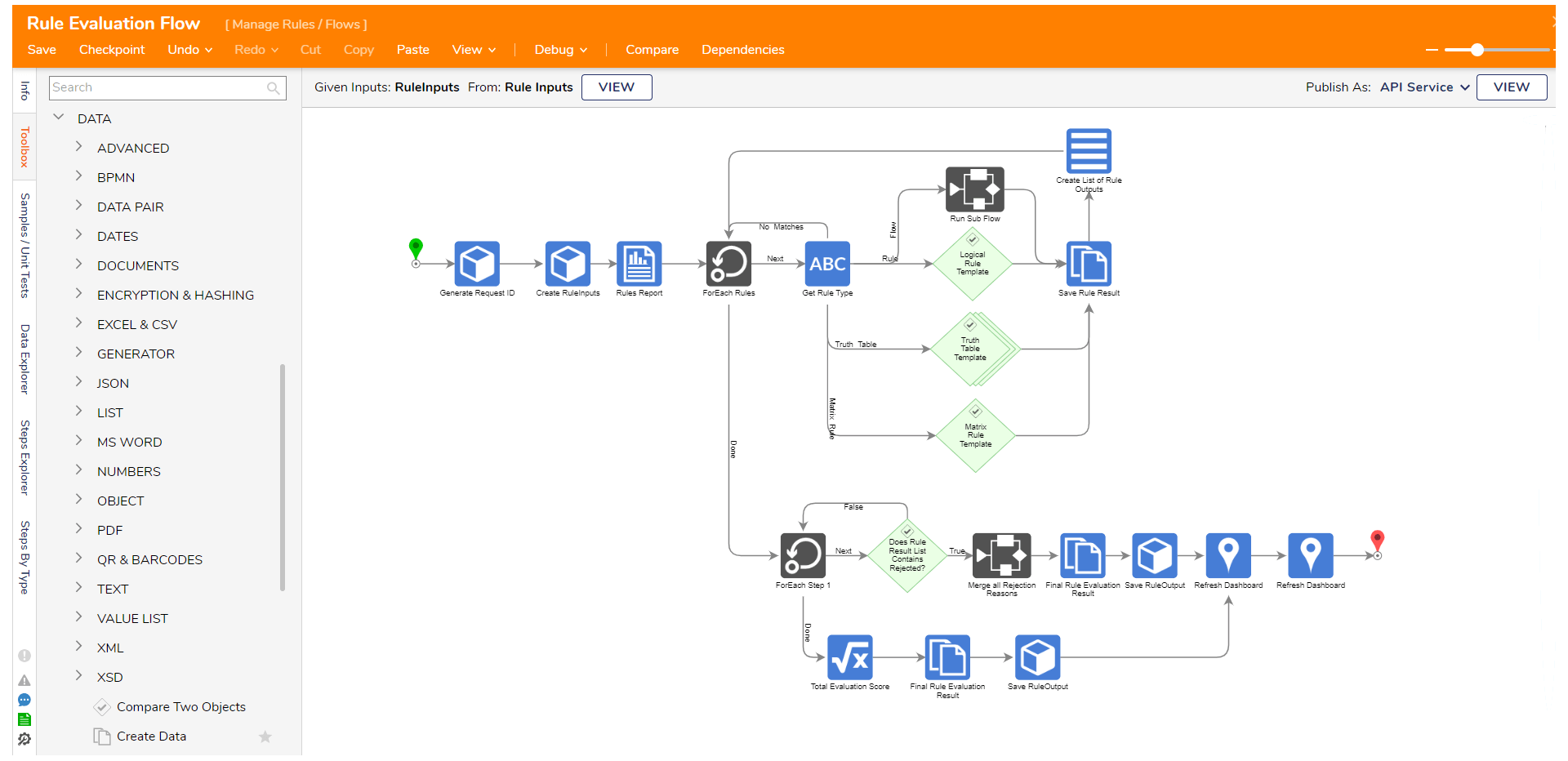
Whether you need to convert Word documents into PDFs or generate automated reports, our workflow library offers over 3,000 specialized actions and interactions to choose from. If something is missing, use our developer SDK to create your own custom steps.
With real-time insights into your processes, you can identify bottlenecks and inefficiencies, and make data-driven decisions to improve your operations. Decisions is the quickest way to build software and solve your most difficult problems. Book a demo to learn how we can quickly deliver software to simplify and standardize your business operations.

This website use cookies to help you have a superior and more relevant browsing experience on the website. Privacy Policy